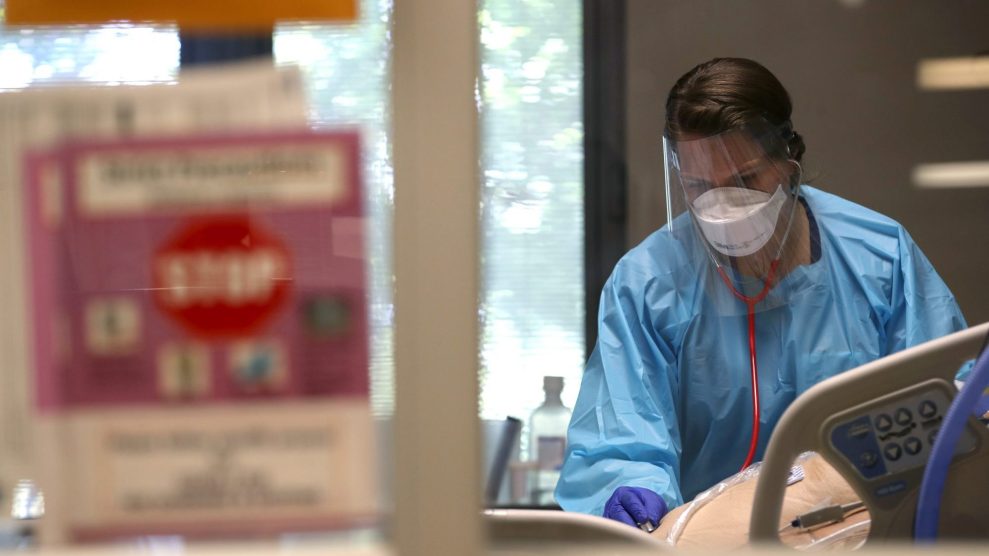
A nurse evaluates a coronavirus COVID-19 patient in an intensive care unit (ICU).Justin Sullivan/Getty
Holly Valentine, a nurse practitioner in a practice specializing in cosmetic surgery, had not worked in an ICU for four years. But in early March, after hospitals paused most elective surgeries because of the novel coronavirus pandemic, she called her former hospital manager and asked for shifts at Our Lady of the Lake Hospital in Baton Rouge, Louisiana. As the major medical center in the region, Our Lady of the Lake Hospital was bracing for an onslaught of COVID-19 patients from all over the area. “He said I could start tomorrow,” Valentine recalls.
In March and April, as COVID-19 overwhelmed some healthcare systems across the country, hospitals desperately sought additional nurses to serve infected patients. Some, like Our Lady of the Lake, were able to reorganize workers from within their own facilities and pull in local reinforcements like Valentine, bumping pay by $20 an hour for nurses working with infected patients.
Desperate to shore up their staff, other hospitals and healthcare systems hired reinforcements through independent staffing agencies that recruited nurses from all over the country, offered them sometimes breathtaking amounts of money, and sent them to virus hotspots. As this unfolded, the complex, often fragile relationship among medical personnel, healthcare systems, and the staffing companies that sometimes broker the relationships between the two has been stressed like never before.
“Not everybody is going to quit to chase hazard pay,” says Joanne Spetz, a health economist and associate director of research at Healthforce Center at the University of California-San Francisco. But only a handful of nurses need to leave for travel nurse contracts to spike a hospital’s costs, and bumping their pay to maintain their staff has turned out to be a necessary strategy to keep them around. “It may be a better deal to pay the extra money now than the even higher travel nurse rate that you’d have to pay for those who slip out the door.”
When New York City hospitals faced an onslaught of coronavirus patients in March and April, New York City Health and Hospitals, which was responsible for deploying staff to public hospitals throughout the city, expanded its capacity by hiring thousands of travel nurses at often astonishing rates—up to $13,000 a week, more than six times the average pay. Nurses arrived from all over the country to work. Northwell Health, a 23-hospital network that covers New York City and Long Island, and the largest private employer in the state, hired hundreds of short-term travel nurses from staffing agencies to prevent hospitals from being overwhelmed by unprecedented demands. Under normal circumstances, Northwell Health, with a $12 billion annual operating budget, employs 69,000 people—about a quarter of them nurses.
After state governor Andrew Cuomo called for hazard pay in mid-April, some healthcare providers began offering their frontline employees extra benefits. In Northwell Health’s case, some medical workers received a $2,500 pay bump and extra paid time off. But at the same time, rates for travel nurses far exceeded what these hospitals were able to offer their regular staff, which could have posed a potential problem for hospitals hoping to not lose staff to once-in-a-lifetime travel pay.
Under normal circumstances, a travel nurse might replace a hospital staffer who goes on leave, say, for a family emergency or the birth of a child. Staffing agencies are frequently called upon to send nurses to crisis zones when a natural disaster strikes. Sometimes travelers are used for union-busting during work stoppages. Hospitals coping with the demands from the pandemic who turned to staffing agencies needed lots of specialized nurses for lengthy periods of service, while being forced to pay them the high rates usually reserved for short-term deployment. Northwell Health, which hired more than 500 nurses from nurse staffing agencies during the height of the pandemic, anticipates keeping 250 of them on the payroll through June. When I asked Maureen White, chief nurse executive for the network, about the high price tag, she told me, “We believe very strongly that if you do what’s right for the patient, it will be what’s right for your bottom line. And so, we did not look at the bottom line.”
In some parts of the country, where the spread of the coronavirus has been less intense, many nurses have been furloughed by hospitals that had stopped elective procedures. For them, the uncertain economic outlook makes travel nursing and its lucrative pay more attractive than ever. Other healthcare providers are trying to avoid furloughing or terminating their own employees, even though income from elective surgeries remains frozen. Experts on the economics of healthcare see healthcare systems forced into a dangerous guessing game that threatens public health and the solvency of the hospitals trying to provide it.
The best-case scenario for a hospital anticipating a crush of COVID-19 patients would be for it to expand its medical personnel to cover ICU and critical units, either by hiring help or reassigning its existing staff, and then reorienting the space and equipment to increase the number of beds, wards, and medical devices to absorb the new patients. If the local community practiced social distancing and effectively flattened the curve, the hospital would have taken a number of costly steps that proved to be unnecessary. “You’re all dressed up for the prom and the date didn’t show,” is the way Spetz describes it.
In Seattle, the University of Washington Medical Center is an example of that almost best-case scenario. The virus may have first appeared in the US there in late January—though difficulty in tracking leaves scientists and officials uncertain of pinpointing the timing and location. UWMC acted fast, and with a combination of increased healthcare spending and effective quarantining by the community, the severity of the outbreak was contained. The hospital was not overrun by COVID-19 patients, and enough staff was there to provide services. Then came the consequences: Nearly four months after the first cases were reported, on May 18, UWMC announced a $500 million budget shortfall and furloughed 1,500 of its 30,000 employees.
During a press conference announcing the cuts, UW Medicine’s chief health system officer Lisa Brandenburg explained what had happened. First, “we cancelled all elective procedures,” she said. “The second is that we had increased expenses of caring for COVID-19 patients.” Now the hospital plans to return to the elective procedures that had sustained the organization. “I don’t wish trauma or burns or solid organ transplants on anyone, but that’s what these hospitals are built to do,” Dr. John Lynch, medical director of employee health at the university’s Harborview Medical Center, told me. “The way it’s set up financially, we need those patients to do our job, to keep the hospitals viable. It sounds completely morbid, I understand that.”
As Spetz noted, “This thing has absolutely laid open for everyone to see how the hospital financing structures have all of these perverse incentives in it.”
For hospitals that had contracted with nurse staffing agencies to prepare for COVID-19 patients, the hazard pay rates added to the economic burden from the epidemic that’s still unfolding. During the last few months, “we’ve seen a huge shift in demand and migration,” says Martin Vidal, the CEO of Trusted Nurse Staffing, a Buffalo, NY-based travel nurse company. “When you see pay rates at three times what [nurses] normally see, that means our bill rates are the same. Are these hospitals going to be able to pay that?”
Typically, paying for travel nurses isn’t a problem; they’re contracted on an individual and temporary basis. Since the industry emerged in the 1970s, it has grown to encompass almost 100,000 nurses and hundreds of staffing agencies. According to a 2018 survey by the federal government, travelers make up around 2.6 percent of the nursing workforce. In 2012, nurse staffing was estimated to be a $3.6 billion industry with potential growth to $5.3 billion by 2018. Spetz says a combination of factors were already beginning to threaten travel nurse agencies over the last few years: A nationwide nurse shortage was showing signs of improvement, healthcare providers increasingly turned to local resources to avoid agencies’ transaction fees, and disruptive tech start ups began to offer the same service of matching hospitals with nurses for less money. Then COVD-19 revived the hospitals’ need for major reinforcements—fast.
The wide-scale furloughing of nurses in less-affected regions, especially those who work outside of trauma wards, created a large available workforce at just the time when there was an increased need for intensive and clinical nurses in hard-hit regions like New York City and Detroit. It might sound like a problem that solves itself: Nurses are furloughed in some places because procedures were paused as a result of the health care emergency, and that, in turn, created a supply of nurses for hospitals buckling under the strain of new cases because of the health care emergency. But not all nurses have the same skill sets and specialties that hospitals facing overwhelming demands from COVID-19 patients required.
“It’s an imbalance in the whole market,” says Spetz. “This new cohort is looking for travel temp work, and there’s a sudden demand, but the demand is not broad-based. The need is for people comfortable with ventilators, in ICUs and emergency departments. This is a double mismatch.”
Both healthcare providers and staffing agencies have turned to the Joint Commission, a healthcare evaluation organization that credentials both, to assess each other’s quality. For the last decade Northwell Health—one of the 22,000 providers whose facilities the Joint Commission accredits—has relied on Cross Country Nurses, in part because it’s one of the 450 staffing agencies that’s also certified by the Joint Commission. However, on March 16, the commission suspended its evaluation practices, to “allow health care organizations and professionals to focus on preparing and caring for patients with COVID-19,” Joint Commission Maureen Lyons wrote in an email.
In March and April, NYCHH needed still more personnel, despite concerns about a lack of personal protective equipment for healthcare workers. Vidal says he saw hospitals and healthcare systems begin to loosen requirements. “Hospitals were taking in anyone they could,” he says. “They didn’t need OR nurses, they needed anyone with a nursing license, period.”
In early March, Krucial Staffing, a Kansas-based travel nurse company that is not certified by the Joint Commission, contracted with New York City Health and Hospitals and began sending thousands of healthcare workers to hospitals slammed by COVID-19. Krucial was offering three-week contracts of up to $13,000 a week. I asked Julie Aultman, a medical ethicist at Northeast Ohio Medical University, if she’d ever seen similar pay rates in the world of nurse staffing. “The only time I’ve ever seen [rates] like that,” she replied, “is people trying to get college-aged women to donate their ova.”
Some nurses who contracted with Krucial ultimately regretted their decision. A lawsuit filed by seven former Krucial-hired nurses alleges “unsafe” clinical conditions where PPE was unavailable and nurses were asked to perform work beyond their scope of training, endangering themselves and patients. “There’s death and dying everywhere you go. There are no ventilators, no gloves, nothing,” Jose Pinlac, a nurse named in the lawsuit, told me. “It [was] like a war zone.” Another nurse, Mindy Evangelisti, who was contracted with Krucial but isn’t listed in the suit, said, “People were getting thrown into that who had just gotten out of nursing or PA school. So it’s unfair to the individual—and probably to the patients.”
Krucial Staffing did not respond to requests for comment on this story.
When Valentine arrived for work at Our Lady of the Lake in Baton Rouge, the hospital had converted three floors into a mass ICU to accommodate more than 250 seriously ill COVID-19 patients, many on ventilators; the pediatric unit was converted for those in recovery. Orthopedic, operating room, or recovery ward nurses in the hospital were moved to the trauma floors. In some cases, ICU nurses were paired with those pulled from other specialties, operating in small teams, to ensure things ran smoothly. “This was a total seat of the pants situation—out of necessity,” she says. By the end of April, the patient surge had subsided.
New York City found itself on a similar timeline. On May 19, the city reported 993 new cases, down from more than 3,700 two months earlier. The Krucial Facebook page, from which the company once broadcasted recruitment ads for hundreds of nurses at a time, is now dominated by posts celebrating the heroism of nurses. “Looking back, what are some of your favorite memories on deployment?” one post asks followers.
COVID-19, however, isn’t over. To make up for lost time, hospitals are beginning to resume the elective surgeries that provide essential income. With public health experts predicting potentially more devastating waves of the pandemic in the fall, there’s not a moment to lose.
“So now we’ve bought some time,” says Spetz. With it, she says, the industry of healthcare can start to reshape itself in preparation for the next surge—whether its COVID-19 or something else. The recent experience of this epidemic, however, has forced health care institutions to face a key question: Should they find the most efficient way to import travelers with ICU experience, or build a more flexible network from within their own personnel rosters, which might result in reducing travel nursing into a much smaller operation? “That’s a debate that’s above my pay grade,” she says.