<a href="http://www.flickr.com/photos/soldiersmediacenter/9971779476/">US Army</a>/Flickr
This story first appeared on the TomDispatch website. The text of this piece is an excerpt, slightly adapted, from Ann Jones’s new book They Were Soldiers: How the Wounded Return from America’s Wars—The Untold Story, just published by Dispatch Books/Haymarket Books
In 2010, I began to follow US soldiers down a long trail of waste and sorrow that led from the battle spaces of Afghanistan to the emergency room of the trauma hospital at Bagram Air Base, where their catastrophic wounds were surgically treated and their condition stabilized. Then I accompanied some of them by cargo plane to Ramstein Air Base in Germany for more surgeries at Landstuhl Regional Medical Center, or LRMC (pronounced Larm-See), the largest American hospital outside the United States.
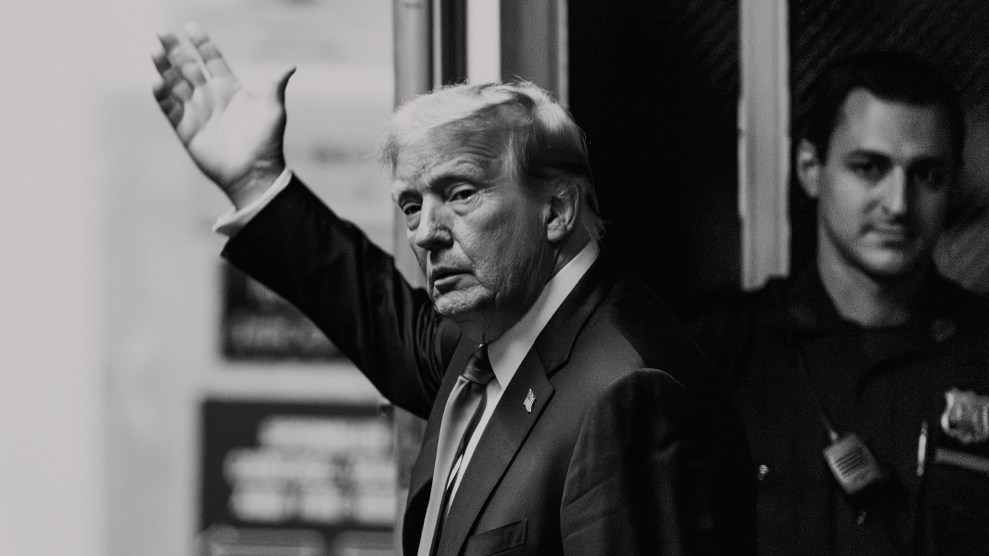
![]() Once stabilized again, those critical patients who survived would be taken by ambulance a short distance back to Ramstein, where a C-17 waited to fly them across the Atlantic to Dover Air Base in Delaware. There, tall, multilayered ambulances awaited the wounded for the last leg of their many-thousand-mile journey to Walter Reed Army Medical Center in Washington D.C. or the Naval Hospital at Bethesda, Maryland, where, depending upon their injuries, they might remain for a year or two, or more.
Once stabilized again, those critical patients who survived would be taken by ambulance a short distance back to Ramstein, where a C-17 waited to fly them across the Atlantic to Dover Air Base in Delaware. There, tall, multilayered ambulances awaited the wounded for the last leg of their many-thousand-mile journey to Walter Reed Army Medical Center in Washington D.C. or the Naval Hospital at Bethesda, Maryland, where, depending upon their injuries, they might remain for a year or two, or more.
Now, we are in Germany, halfway home. This evening, the ambulance from LRMC heading for the flight line at Ramstein will be full of critical-care patients, so I leave the hospital early and board the plane to watch the medical teams bring them aboard. They’ve done this drill many times a week since the start of the Afghan War. They are practiced, efficient, and fast, and so we are soon in the air again. This time, with a full load.
Two rows of double bunks flank an aisle down the center of the C-17, all occupied by men tucked under homemade patchwork quilts emblazoned with flags and eagles, the handiwork of patriotic American women. Along the walls of the fuselage, on straight-backed seats of nylon mesh, sit the ambulatory casualities from the Contingency Aeromedical Staging Facility (CASF), the holding ward for noncritical patients just off the flight line at Ramstein.
At the back of the plane, slung between stanchions, are four litters with critical care patients, and there among them is the same three-man CCAT (Critical Care Air Transport) team I accompanied on the flight from Afghanistan. They’ve been back and forth to Bagram again since then, but here they are in fresh brown insulated coveralls, clean shaven, calm, cordial, the doctor busy making notes on a clipboard, the nurse and the respiratory therapist checking the monitors and machines on the SMEEDs. (A SMEED, or Special Medical Emergency Evacuation Device, is a raised aluminum table affixed to a patient’s gurney.) Designed to bridge the patient’s lower legs, a SMEED is now often used in the evacuation of soldiers who don’t have any.
Here again is Marine Sergeant Wilkins, just as he was on the flight from Afghanistan: unconscious, sedated, intubated, and encased in a vacuum spine board. The doctor tells me that the staff at LRMC removed Wilkins’s breathing tube, but they had to put it back. He remains in cold storage, like some pod-person in a sci-fi film. You can hardly see him in there, inside the black plastic pod. You can’t determine if he is alive or dead without looking at the little needles on the dials of the machines on the SMEED. Are they wavering? Hard to tell.
Flight Risk
The CCAT team has three other critical patients to think about. They are covered with white sheets and blankets, but it’s easy to see that the second patient is missing both legs. His right hand is swathed in thick bandages, almost as fat as a football. His face is ripped and torn so that his features appear to be not quite where they belong, but pushed up and to one side—his nose split and turned askew. He’s sedated and on a ventilator meant to assist his breathing, but his chest convulses as he struggles with the job.
 The respiratory therapist hovers, checking monitors, adjusting a breathing tube, and the man quiets. But not for long. The IED blast that took off both his legs above the knee bypassed his pelvis to slam into his chest. He must have been doubled over, crouching, when he walked onto the bomb. The impact damaged his lungs in ways not yet fully understood, so that now when he breathes on his own, every breath costs him more than he has to give.
The respiratory therapist hovers, checking monitors, adjusting a breathing tube, and the man quiets. But not for long. The IED blast that took off both his legs above the knee bypassed his pelvis to slam into his chest. He must have been doubled over, crouching, when he walked onto the bomb. The impact damaged his lungs in ways not yet fully understood, so that now when he breathes on his own, every breath costs him more than he has to give.
The CCAT team confers. To stop the convulsive effort to breathe, the doctor can paralyze him and let the ventilator do the work of respiration, but that means removing from his intestine the feeding tube pumping in the calories he needs to heal these catastrophic wounds. It’s a fine line, and the team walks it for the next hour until it’s clear the man needs rest more than nourishment. Then the doctor administers a drug, the body grows still as stone, and the soldier inside sleeps softly while the ventilator steadily breathes in and breathes out.
Patient number three is breathing on his own and fast asleep, a saline drip feeding into his arm. He looks okay, but for the flattening of the blanket under the SMEED. He’s lost both legs, but both below the knee. He has his hands. He has his junk. Of these four patients, he’s the one the military and the media will call “lucky.” But the doctor doesn’t call him that. He says, “You can’t assess his injuries in comparison to those of other soldiers who happen to be on the same plane. You have to assess them in comparison to who he was before.” He is a boy who used to have legs and now he doesn’t.
The fourth CCAT patient is a darkly handsome kid who lost both legs to an IED. His right arm ends in a bulbous bandage, but something about its shape suggests the hand might still be all there. He’s conscious and breathing on his own, vaguely gazing at a thin woman in blond boots and a light jacket who stands next to his litter and clutches at the rail as if to hold herself upright.
She was called to LRMC because her son was close to death, but she is now taking him home, what’s left of him, alive. In the dim light, she looks dazed, but she leans over him and speaks into his ear and soon he sleeps. The doctor tells me that the boy, a Marine, lost one leg below the knee, and the other very high up—too high for him to wear a prosthetic leg.
“He’ll be in a wheel chair,” the doctor says. “It’s doubtful he’ll ever walk. His right arm is all there, but the hand is blasted. He’ll probably lose his fingers at least, but he may have enough of a hand left to power a wheel chair on his own. It’s hard to say. He lost one testicle, too, and part of the penis and urethra. But he could still be fertile. There’s a chance.”
The cavernous plane is very cold. There’s a blanket on each of the seats along the wall. I wrap myself up and sit down next to my military minder Sergeant Julian, mainly to stay out of the way of the CASF nurses who are busy checking on their patients, getting those on the bunks well settled for the long flight. The mother of the handsome kid has also sunk into a seat next to her son’s litter, but she leans forward, still clutching the bedrail as if to hang on to her boy. She has thrown a blanket around her like a cape, but even at a distance I can see that she’s cold. I pick up a spare blanket and take it to her. She looks up as I hold it out to her wordlessly in the deafening plane. “I’m fine,” she says, loudly enough for me to hear.
“Your son?”
“He’s fine.” She looks at him and changes tense. “He’s going to be fine.”
“That’s good,” I say.
“He’s alive. He almost wasn’t, but he’s alive. He’s fine.”
I offer the blanket again. “Take it. Keep warm.”
Later I notice that she has made a cocoon of the blankets and slumped over the adjacent seat to sleep. Only toward the end of the flight, when she must be feeling some relief that her son is going to survive it, does she begin to tell me about him. She got word of his injury when he was still in the field hospital in Helmand Province, and she arrived at LRMC from southern California the same day he was brought in from Bagram. Three days later, miraculously, she is bringing him home. Well, not home really, but to the States anyway, to the Naval hospital at Bethesda, Maryland.
Her son has an older brother who deployed once to Iraq and once to Afghanistan and now is safe at home in California. But this boy, a Marine, had a training accident that left him with a head injury requiring brain surgery. He was medically discharged, but reenlisted and was deployed to Afghanistan. He had been there two months when his unit was assigned to clean up an area another unit had officially cleared of Taliban. You remember the policy: clear, hold, and build. They were doing the hold part when he stepped on the IED. The other Marine, the one who can’t breathe, was hit by the same blast, or maybe another one at the same time. “They told me how it happened,” she says, “but I don’t think I heard.”
Months later, I will call her in California to see how her son is getting along. He’s still in the hospital. They’re still working on his wounds. He’s not doing any rehab yet. But the military moved him to San Diego so she and her husband can visit him often. She says he’s doing “fine,” though it will still be many months before he can come home.
In the meantime, her contractor husband has enlisted his friends to help widen doorways, lower light switches, build ramps, and reconstruct a bathroom on the ground floor for a boy in a wheelchair. It’s a weekend and I can hear them hammering as we talk on the phone. “They say he’ll always be in a wheelchair,” she says, her voice shaking. “I was in our pool this morning, and I realized that he’ll never be able to get into it by himself. He loves the pool.” I stay on the line, listening to her cry. She says, “He’s a beautiful swimmer.”
“Everything Still Hurts…”
On the plane I talk to some of the ambulatory patients sitting along the walls, wrapped in blankets like so many Pashtuns. Most are hurt just enough to have to be out of action for a while. One boy got a boot caught in the door of an armored vehicle, an MRAP, that wasn’t moving at the time. It’s a long way down from the passenger seat. He broke his arm. He blurts this out, then tells me he worries about what he’s going to say back at his home base. “I can’t tell them I just fell out.”
Another kid dropped a barbell in the gym and broke some bones in his foot. Two others hadn’t recovered from chronic back pain and muscle spasms induced by carrying too much weight. Doctors sent them back downrange to their units two or three times and each time they broke down again. The painkillers had only left them dazed. One says, “Everything still hurts, and you can’t remember what you’re doing, so it makes you nervous. So now they’re sending me home because I guess maybe the pain doesn’t make you so nervous in the US of A.”
One young man collapsed while jogging at a base in the Persian Gulf. “I need a new valve in my heart,” he says, “so they’re sending me home to get it done there. I’m really lucky they found it. The Army saved my life.” His wife sits beside him, wearing a brand new Frankfurt sweatshirt and a bracelet dripping with gnomes. While the doctors at LRMC assessed her husband’s cardiac function, she went shopping. She tells me confidentially, “I for sure didn’t want to sit around any old hospital.”
An older Army officer calls me over and gestures toward the empty seat by his side. He sits ramrod straight, wrapped in his blanket, and speaks through tight lips as if he fears what might come out of his mouth. “I’ve been in the Army twenty-six years,” he says, “and I can tell you it’s a con.”
He has been an adviser to the chief counterterrorism officer in Iraq. It’s hard even to imagine what’s involved in work like that, but his version of his job description evidently failed to match the official checklist of his boss. He doesn’t think much of military bosses or politicians or Americans in general who send the lowliest 1% to fight wars that make the other 1%, on the high end, “monu-fuckin’-mentally rich.”
He says he’s going home for “psych reasons” caused by “life,” and he is never going to deploy again. He has two sons, 21 and 23, in college, “They won’t have to serve,” he says. “Before that happens, I’ll shoot them myself.”
I ask if he has any particular reason to dislike the military so intensely. “War is absurd,” he says. “Boys don’t know any better. But for a grown man to be trapped in stupid wars—it’s embarrassing, it’s humiliating, it’s absurd.”
TomDispatch regular Ann Jones is the author of a new book, They Were Soldiers: How the Wounded Return from America’s Wars—the Untold Story, a Dispatch Books project in cooperation with Haymarket Books. Andrew Bacevich has already had this to say about it: “Read this unsparing, scathingly direct, and gut-wrenching account—the war Washington doesn’t want you to see. Then see if you still believe that Americans ‘support the troops.'” Jones, who has reported from Afghanistan since 2002, is also the author of two books about the impact of war on civilians: Kabul in Winter and War Is Not Over When It’s Over. This article is an excerpt from her new book.
Follow TomDispatch on Twitter and join us on Facebook or Tumblr. Check out the newest Dispatch Book, Ann Jones’s They Were Soldiers: How the Wounded Return From America’s Wars—The Untold Story To stay on top of important articles like these, sign up to receive the latest updates from TomDispatch.com here.